
Australian Medical Association gets vaping completely wrong…again
Posted on January 17, 2023 By Colin
THE AUSTRALIAN MEDICAL ASSOCIATION's submission to the TGA Consultation on vaping nicotine is an evidence-free zone. It is based on denial of the scientific evidence and the huge benefits that vaping offers to public health. Their proposal for regulation will lead to increased criminal supplies and more smoking deaths in Australia.
Australia has the most restrictive policy on vaping of all western countries and this has been a resounding failure.
the AMA President proposes doubling down with "stronger, strictly enforced regulations on vaping", the very approach which has created the current debacle
This will only compound the current failure and push unregulated vaping products further underground.
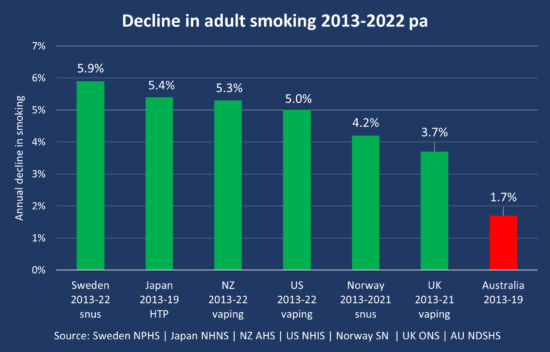
The AMA has dismissed the lifesaving benefit of vaping to adult smokers, with the President saying that vaping is "not part of tobacco control". In fact, vaping is the most effective aid for quitting smoking. In countries where vaping and other harm reduction strategies are widely available, the smoking rate over the last decade has declined 2-3 times faster than in Australia, and vaping is a major contributor.
Some of the more serious flaws in the AMA submission are listed below.
Continuation of the prescription-only model
The prescription model has been a an embarrassing failure. Fewer than 1% of doctors are publicly listed as nicotine prescribers and less than 10% of vapers have a nicotine prescription.
The prescription model has diverted users to a thriving black-market where unregulated and incorrectly-labelled products are freely sold to adults and young people.
As a result, there has also been a substantial growth in youth vaping
Nicotine liquid is an adult consumer product, like cigarettes and alcohol. It is not a medicine and should not require a prescription, especially when deadly cigarettes are widely available at every corner shop.
The optimal approach is for vaping products to be sold by licensed retailers with strict age verification and improved safety standards. This model is working successfully in other western countries, such as New Zealand and the United Kingdom.
'lack of evidence as an effective nicotine cessation tool'
WRONG. There is now "high certainty" evidence that vaping is significantly more effective as a quitting aid than nicotine replacement therapies (NRT) such as nicotine gum and patch, according to the latest Cochrane review, the gold standard for testing whether treatments work.
A recent analysis by the UK National Institute for Health Research concluded that vaping was the most effective single therapy, followed by varenicline (Champix) and NRT.
Importantly, vaping is the most popular quitting aid in Australia and globally and is likely to have a far greater reach and impact on smoking rates than any other strategy.
"Vaping products are a gateway to smoking for young people"
WRONG. Young people who try vaping are more likely to later try smoking. However, this does not mean that vaping causes them to take up smoking if they would not otherwise have done so anyway (the gateway hypothesis).
A more plausible explanation is a 'common liability' for risk-taking, ie that some young people are more likely to vape and smoke due to shared shared risk factors, such as inherited, personal or social causes.
If the gateway hypothesis was true, increased vaping would lead to increased cigarette smoking among youth. However, increases in youth vaping have been accompanied by an accelerated decline in youth smoking since vaping became popular, for example in the US:
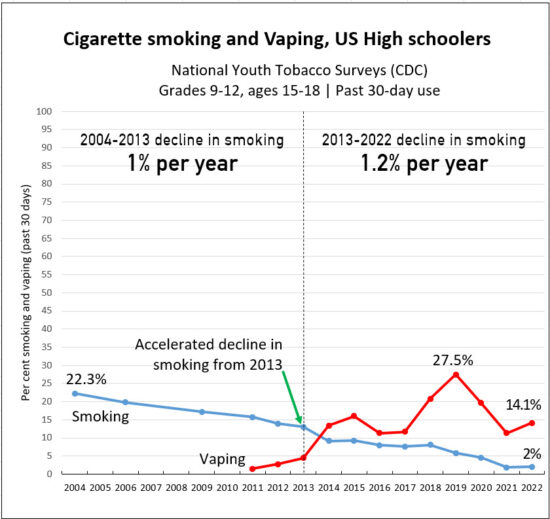
This and other studies suggest that vaping and smoking are substitutes and that vaping is diverting young people away from smoking. Young people should do neither, but it is better if they vape than smoke.
“reduce the nicotine concentration from 100mg/mL to 20mg/mL”
Excessively low doses of nicotine will lead to lower rates of switching. Smokers often need higher doses of nicotine in the early stages of switching or while they are learning to vape. Heavier or more dependent smokers may find e-cigarettes unsatisfying with low dose nicotine liquids– so those most at risk are denied the products more likely to work.
Higher concentrations of nicotine are safer than low concentrations as they generate smaller vapour volume, with a corresponding reduction in toxicants. Furthermore, users titrate their nicotine intake to control their exposure.
A reduction to 50mg/mL is a reasonable compromise as this concentration is required for many popular disposable and more compact pod devices. The smaller size, convenience and nicotine delivery of these devices has made them very popular as transition models.
Overdosing from nicotine e-liquids is rare and usually results in minor symptoms of short duration. Most accidental poisoning cases are preventable with strategies such as child-proof packaging and safety warnings.
"there are significant risks from vaping "
WRONG. Vaping is an adult quitting aid or substitute for smoking. Although not risk-free, vaping is a substantially safer than smoking. Switching completely to vaping dramatically reduces toxicant exposure and biomarkers of harm (toxins found in the body) and improves symptoms and clinical outcomes.
The precise long-term risks of vaping will not be known for decades but they are highly likely to be far less harmful than smoking
After 15 years, serious effects from vaping nicotine have been extremely rare and there has never been a death from vaping.
Vaping nicotine does NOT cause 'popcorn lung' or 'EVALI' as claimed by the AMA
“all vaping flavours should be restricted”
Flavour bans can be counterproductive. For example, a 2020 flavour ban in San Francisco resulted in more than doubling of smoking by high school students, and an increase in smoking in young adults. After a ban on pod-based flavours in the US in 2019, 14% of vapers reported returning to smoking.
Flavours are an integral part of the appeal of vaping for adult smokers and play an important role in the initiation of vaping for current smokers. Flavoured e-liquids also increase quit rates compared to non-flavoured or tobacco flavours and reduce the rate of relapse. Those who vape with flavours also have higher odds of making a quit attempt.
Reasonable recommendations for flavours are
- Simple descriptions of flavour profiles only eg ‘mint’, ‘blueberry’, ‘tobacco’, ‘vanilla tobacco’
- Prohibit descriptive flavour names that specifically appeal to youth eg ‘dragon vomit’
- Prohibit flavours found to have a material risk to health
“Only a patient's usual doctor can prescribe nicotine”
As <1% of GPs prescribe nicotine, this would make it almost impossible for smokers and vapers to legally access nicotine liquid for vaping and would amount to an almost complete prohibition of vaping.
'Registration of all products on the ARTG'
The AMA wants all nicotine vaping products to go through, expensive and onerous medicines regulation, while deadly cigarettes remain virtually unregulated. Medicines regulation will increase cost, introduce delays and stifle innovation. Only tobacco companies and a small number of large companies have the resources to comply with this requirement. No other western country treats nicotine for vaping solely as a medicine and none requires a doctor’s prescription.
However, vapes are not medicines, they are consumer products. Vaping is about replacing one pleasurable consumer behaviour with another far less harmful one
Vaping nicotine should be regulated by the Australian Competition and Consumer Commission like other consumer products.
'The Personal Importation Scheme must cease'
The AMA wants to ban personal imports to improve quality standards. However this can be achieved by a more stringent regulation system as in the UK and NZ in which manufacturers must meet a set of approved standards before marketing.
The AMA President
The AMA President is displaying gross hypocrisy in supporting this policy. Dr Robson was a supporter of vaping before he became AMA president, but appears to have been forced to toe the party line.
In 2015 he wrote an article in favour of vaping and has expressed positive views since then. However when he became AMA president he took on the draconian AMA position.
We have politely requested a meeting to discuss vaping with Dr Robson on three occasions, but all requests have been ignored.
It appears that Dr Robson is now putting the AMA ideology and politics before public health and scientific evidence.